|
|
Sacrococcygeal Chordoma
General Considerations
- Rare primary malignancy of bone
- Originates from embryonic remnants of the notochord
- Location
- 40% of all sacral tumors
- Most common in 4th or 5th sacral segment
- 35% at skull base around clivus
- Benign tumors but may locally invade and compress
- 15% in remainder of spine
- Cervical spine most common
- Occurs between the ages of 30-70 with a 2:1 male:female ratio
Clinical Findings
- Low back pain is most frequent symptom (70%)
- Constipation or fecal incontinence
- Rectal bleeding
- Sciatica from nerve root compression
- Frequency, urgency, straining on micturition
Imaging Findings
- Large presacral mass (>10cm) with displacement of the rectum and/or bladder
- Solid tumor with cystic areas in 50%
- Destroys multiple sacral and coccygeal segments
- Sequestered bone fragments are common
- Sclerotic rim in 50%
- May have amorphous calcifications, especially peripherally
- May cross the sacroiliac joint
- CT findings
- CT is helpful in defining bone destruction and calcification within lesion
- With contrast, the pseudocapsule may enhance
- Usually low attenuation soft tissue mass with destruction of the sacrum and/or coccyx
- May show sequestered bone fragments or calcifications within tumor
- MRI findings
- Modality of choice, especially for clival lesions
- Low to intermediate intensity on T1
- Those lesions that show high signal intensity on T1 have a larger mucinous component
- Very high signal intensity on T2
- Following gadolinium injection, chordomas may show a honeycomb appearance
- Heterogeneous on T1 and T2
- Lesions may rim enhance
Differential Diagnosis
- Plasmacytoma
- Giant cell tumor
- Chondrosarcoma
- Differentiation from chordomas difficult both radiologically and pathologically
- May require immunohistochemical studies
- Metastatic carcinoma
- Lymphoma
Treatment
- All chordomas are relatively radioresistant
- Gamma knife is helpful in sparing adjacent tissues
- Sacral chordomas are usually treated with an en bloc resection of the tumor
- The surgical management of clival tumors is more difficult because of the surrounding structures
Complications
- Metastases in 7-14% of all chordomas; rare with sacral chordomas
- Infection is a frequent complication
Prognosis
- 8-10 years average survival
- Very high (nearly 100%) recurrence rate following surgical removal
 
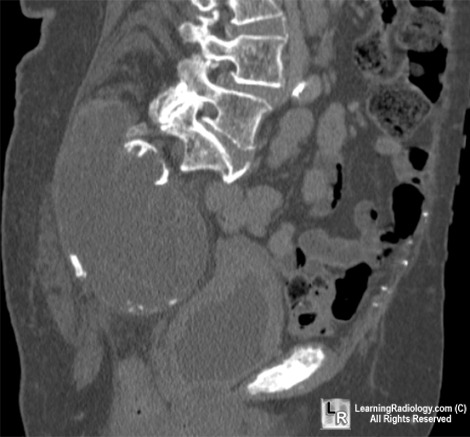
Sacrococcygeal chordoma. (Left) Axial CT scan demonstrates a large soft tissue mass in the pelvis of mixed attenuation containing at least one fragment of bone (black arrow). (Right) Sagittal reformatted CT shows the mass (white arrows) is destroying most of the sacrum and coccyx (red arrow).
For additional information about this disease, click on this icon if seen above.
For same photos without annotations, click here or here
Chordoma eMedicine Authors: Paule Peretti, MD; Hervé Brunel, MD; Frédéric Borrione, MD; Guillaume Gorincour, MD
|
|
|

{kind=link}
{kind=link}